

Atrial Tachycardia Definition & Epidemiology
Atrial tachycardia is a heart rhythm in which the heart beats faster than 100 beats per minute due to an electrical signal in the atria. It is one type of paroxysmal supraventricular tachycardia (PSVT), a term referring to a group of arrhythmias that originate above the atrioventricular junction (AVJ) and that generally begin and end abruptly.1
Collectively, the PSVTs are thought to affect 36 per 100,000 persons per year in the United States. Women are at twice the risk of PSVT compared to men, while older people face a fivefold risk compared with younger people.2,3
Bạn đang xem: Atrial Tachycardia: Diagnosis
Of all PSVTs, atrial tachycardia is the least common, accounting for approximately 1 in 10 cases. Among patients referred for supraventricular tachycardia (SVT) ablation, focal atrial tachycardia (FAT) is present in 3% to 17%.4
Etiology and Risk Factors
In atrial tachycardia, the AVJ is not part of the circuit. This distinguishes it from related arrhythmias such as atrioventricular nodal reentrant tachycardia (AVNRT) and atrioventricular reentrant tachycardias (AVRT).
There are two main types of atrial tachycardia: unifocal and multifocal.
- Unifocal. In the unifocal type, also called focal or ectopic atrial tachycardia, the abnormal electrical impulse begins at a single spot somewhere in either atrium. A subtype of unifocal is called sinus node reentry tachycardia; it involves micro re-entry that arises at the sinus node.
- Multifocal. In multifocal atrial tachycardia (MAT), several areas give rise to these electrical signals.
When FAT arises from reentrant electrical impulses, it is associated with structural heart disease. It may also occur incessantly due to enhanced automaticity in a structurally normal heart, a condition that can result in cardiomyopathy and heart failure.5 Atrial tachycardia commonly occurs after ablation for atrial fibrillation.
By contrast, MAT is closely associated with lung diseases, such as asthma or chronic obstructive pulmonary disease (COPD). It can also result from hypomagnesemia.6
Digoxin and theophylline are among the drugs that can cause atrial tachycardia. Others include β-agonists, phosphodiesterase inhibitors, dobutamine, and milrinone. Substances such as caffeine, cocaine, amphetamines, and alcohol use or withdrawal may also provoke arrhythmia.7
Presentation
Symptoms of paroxysmal supraventricular tachycardia commonly include palpitations, chest pain, fatigue, and/or lightheadedness. Syncope is less common, while sudden cardiac death may rarely occur.
Patients with incessant atrial tachycardia resulting in cardiomyopathy may report heart failure symptoms such as progressive exertional dyspnea. Symptoms of intermittent focal or multifocal atrial tachycardia may relate to underlying heart or pulmonary disease.
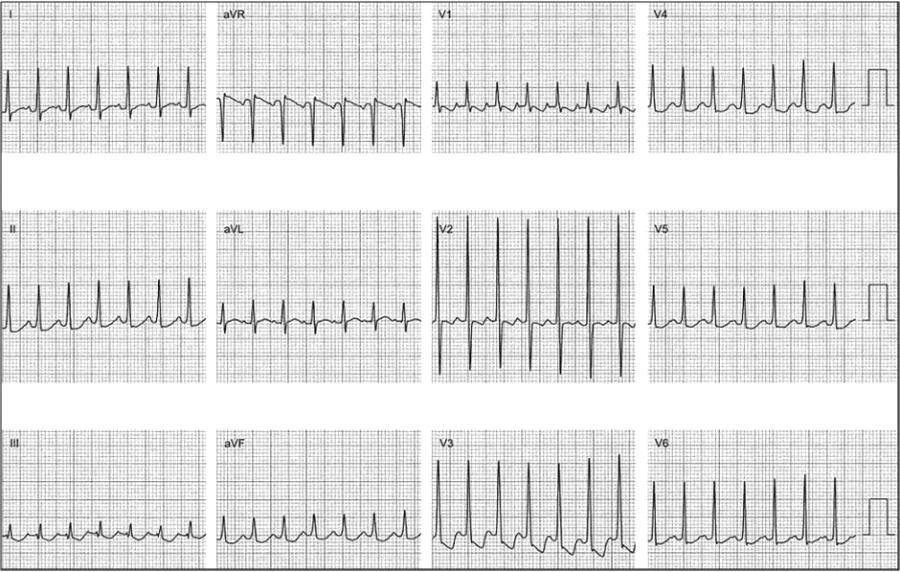
An electrocardiogram (ECG) reveals a regular, narrow-complex tachycardia in which P waves differ from their appearance in sinus rhythm. P waves may sometimes disappear into the preceding T waves.4
Atrial Tachycardia Physical Examination Findings & Workup
Because bouts of tachycardia can be short-lived and episodic, the patient may not be experiencing symptoms during the clinical encounter. The history should elicit a description of episodes, including any triggers; if the episodes occur with activity or amid known heart disease, a ventricular origin may be present. It is also helpful to establish age of onset, abrupt vs gradual onset (the latter suggests sinus tachycardia), and symptom duration.4
The provider should also ask about heart disease, cardiac surgery, and medications, including those that may cause electrolyte disturbance. Inquiries about substance use or withdrawal are important.
Xem thêm : A Complete Guide to Diluting Essential Oils
Physical examination may reveal only tachycardia. If the atria contract against a closed tricuspid valve, blood may backflow into the jugular veins, resulting in visible bulging known as the frog sign.8 (However, the frog sign can also be seen in AVNRT; it is not specific to atrial tachycardia.) Vital signs, including orthostatic blood pressure measurements, may point to other causes of tachyarrhythmia.
For unifocal tachycardia, ECG shows a fast, regular rhythm with isoelectric segments between P-waves. It may be difficult to distinguish from other regular SVTs. The P waves outnumber the QRS complexes, helping to distinguish atrial tachycardia from sinus tachycardia.
With MAT, the ECG shows an irregular rhythm with at least three different P-wave morphologies, typically with isoelectric periods between them.
If the patient is not tachycardic at the time of evaluation, outpatient monitoring may be indicated.4
Some diagnostics can also be therapeutic. Vagal maneuvers such as the Valsalva maneuver or unilateral carotid sinus massage can slow down conduction through the atrioventricular node.9 However, massage should be avoided in older patients with carotid bruits.
Pharmacological interventions such as adenosine, which should be administered in a monitored environment, can also block atrioventricular conduction. If the arrhythmia stops in response to adenosine, it indicates AVNRT or AVRT. With unifocal atrial tachycardia, the ventricular rate will typically slow down in response to adenosine. Transient atrioventricular block with persistent atrial tachycardia suggests a unifocal origin.10
Cardioversion is rarely necessary and is indicated if the patient is hemodynamically unstable and has not responded to other measures. It is not useful to treat MAT.
Laboratory studies should include complete blood count, basic metabolic panel, magnesium, and thyroid-stimulating hormone.10 Patients with known or suspected heart disease may also require measurement of B-type natriuretic peptide and cardiac enzymes.
A chest X-ray may reveal cardiomegaly, while an echocardiogram may reveal structural heart disease.3 In some cases, an invasive electrophysiology study is indicated, especially if ablation of the abnormal atrial impulse(s) is planned. Mapping during such a study can help determine the origin of a unifocal atrial tachycardia.
Differential Diagnosis
The differential diagnosis of narrow-complex tachycardias, including the PSVTs, is important because treatment differs depending on the arrhythmia. This requires scrutiny of the ECG with close attention to P-wave and QRS shapes and to the PR and RR intervals. Practitioners may wish to consult an algorithm to help distinguish atrial tachycardia from other SVTs, including AVNRT, AVRT, permanent junctional reciprocating tachycardia (PJRT), atrial fibrillation, and atrial flutter.3
Briefly, unifocal atrial tachycardia is typically regular, as are reentry tachycardias and sinus tachycardia. By contrast, multifocal atrial tachycardia and atrial fibrillation are irregular. Atrial flutter and atrial tachycardia may also present with variable conduction and irregular rhythm, however.
Unifocal atrial tachycardia’s atrial rate is typically 100 to 250 beats per minute.11 MAT’s isoelectric periods between its three or more P-wave types can help to distinguish it from atrial fibrillation.
Atrial tachycardia and the other PSVTs may be misdiagnosed as panic disorder or anxiety disorder, which may be hazardous if an incessant arrhythmia is overlooked.3
Atrial Tachycardia Prognosis
Xem thêm : When And How To Wean Baby Off Formula
Prognosis depends on the underlying cause. Unifocal atrial tachycardia is usually benign in adults and may not require treatment if it is not sustained. On the other hand, incessant atrial tachycardia can contribute directly to tachycardic cardiomyopathy and reversible heart failure.11The prognosis of MAT will relate in large part to underlying lung disease.Treatment for paroxysmal supraventricular tachycardia includes a variety of antiarrhythmic drugs and/or catheter ablation of the abnormal focus or foci. Unifocal atrial tachycardia may respond to medication; ablation with 3-dimensional mapping technology is frequently successful.
Collectively, the SVTs are thought to be a common reason patients visit a primary care provider or emergency department. However, these arrhythmias seldom result in inpatient admission.
Frequently Asked Patient Questions
What is atrial tachycardia?
Atrial tachycardia is a form of tachyarrhythmia, a heart rhythm in which the heart beats faster than 100 beats per minute due to an electrical signal in the atria. Atrial tachycardia is a type of paroxysmal supraventricular tachycardia (PSVT), a group of arrhythmias that originate above the atrioventricular junction (AVJ).
What is the most common cause of atrial tachycardia?
Drugs that can cause atrial tachycardia include digoxin and theophylline. Other medications include β-adrenergic agonists, phosphodiesterase inhibitors, dobutamine, and milrinone. Substances such as caffeine, cocaine, amphetamines, and alcohol use or withdrawal may also precipitate an atrial arrhythmia.
What is paroxysmal supraventricular tachycardia (PSVT)?
Paroxysmal supraventricular tachycardias (PSVT) are characterized by sudden onset and termination, atrial rates between 140 and 250 beats/min, and normal QRS complexes. The mechanism of PSVTs is most commonly reentry involving the AV node, atrium, or an accessory pathway between an atrium and a ventricle.1
What is unifocal atrial tachycardia?
Unifocal type, otherwise known as focal atrial tachycardia occurs as a result of either automaticity of an atrial ectopic site or reentry. The ECG is that of sinus tachycardia, with a P wave before each QRS complex. But the morphology of the P-wave is different from that of sinus rhythm, demonstrating depolarization of the atrium from an atypical location.1
What is multifocal atrial tachycardia?
In multifocal atrial tachycardia (MAT), the ECG shows an irregular rhythm with at least 3 different P-wave morphologies, and the average atrial rate is >100 beats/min.1 This rhythm most often occurs in the setting of severe pulmonary disease or hypomagnesemia.
Atrial tachycardia vs atrial fibrillation: What is the difference?
An isoelectric baseline between P waves differentiates multifocal atrial tachycardia (MAT) from the chaotic baseline rhythm of atrial fibrillation. Atrial tachycardia commonly occurs after ablation for atrial fibrillation which is a chaotic rhythm with an atrial rate so rapid that P-waves cannot be distinguished on the ECG.1
Atrial tachycardia vs sinus tachycardia: What is the difference?
Abrupt onset of tachycardia is indicative of atrial tachycardia while gradual onset is suggestive of sinus tachycardia. In unifocal tachycardia, the P-waves outnumber the QRS complexes, which helps to differentiate atrial tachycardia from sinus tachycardia.
Atrial Tachycardia ICD 10 Codes
Here are relevant ICD 10 codes for atrial tachycardia:
References
- Helton MR. Diagnosis and Management of Common Types of Supraventricular Tachycardia. Am Fam Physician. 2015;92(9):793-800.
- Orejarena LA, Vidaillet H Jr, DeStefano F, et al. Paroxysmal supraventricular tachycardia in the general population. J Am Coll Cardiol. 1998 Jan;31(1):150-7. doi:10.1016/s0735-1097(97)00422-1
- Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society [published correction appears in Circulation. 2016 Sep 13;134(11):e234-5]. Circulation. 2016;133(14):e506-e574. doi:10.1161/CIR.0000000000000311
- Mahtani AU, Nair DG. Supraventricular Tachycardia. Med Clin North Am. 2019;103(5):863-879. doi:10.1016/j.mcna.2019.05.007
- Liwanag M, Willoughby C. Atrial Tachycardia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022 Jan-.
- Custer AM, Yelamanchili VS, Lappin SL. Multifocal Atrial Tachycardia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022 Jan-.
- Tisdale JE, Chung MK, Campbell KB, et al. Drug-Induced Arrhythmias: A Scientific Statement From the American Heart Association. Circulation. 2020;142(15):e214-e233. doi:10.1161/CIR.0000000000000905
- Velibey Y, Durak F, Türkkan C, Alper AT. “Frog Sign” in paroxysmal supraventricular tachycardia. Anatol J Cardiol. 2018 Apr;19(4):E7. doi: 10.14744/AnatolJCardiol.2018.78045
- Niehues LJ, Klovenski V. Vagal Maneuver. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-.
- Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018;140(8)e382-e482.
- Atrial Tachycardia. Cleveland Clinic. Published 2021. Accessed June 20 2022.
Author Bio
Jenny Blair, MD, is an award-winning journalist and writer based in Vermont.
Updated: 05/28/2024
Nguồn: https://buycookiesonline.eu
Danh mục: Info
This post was last modified on November 26, 2024 10:59 am